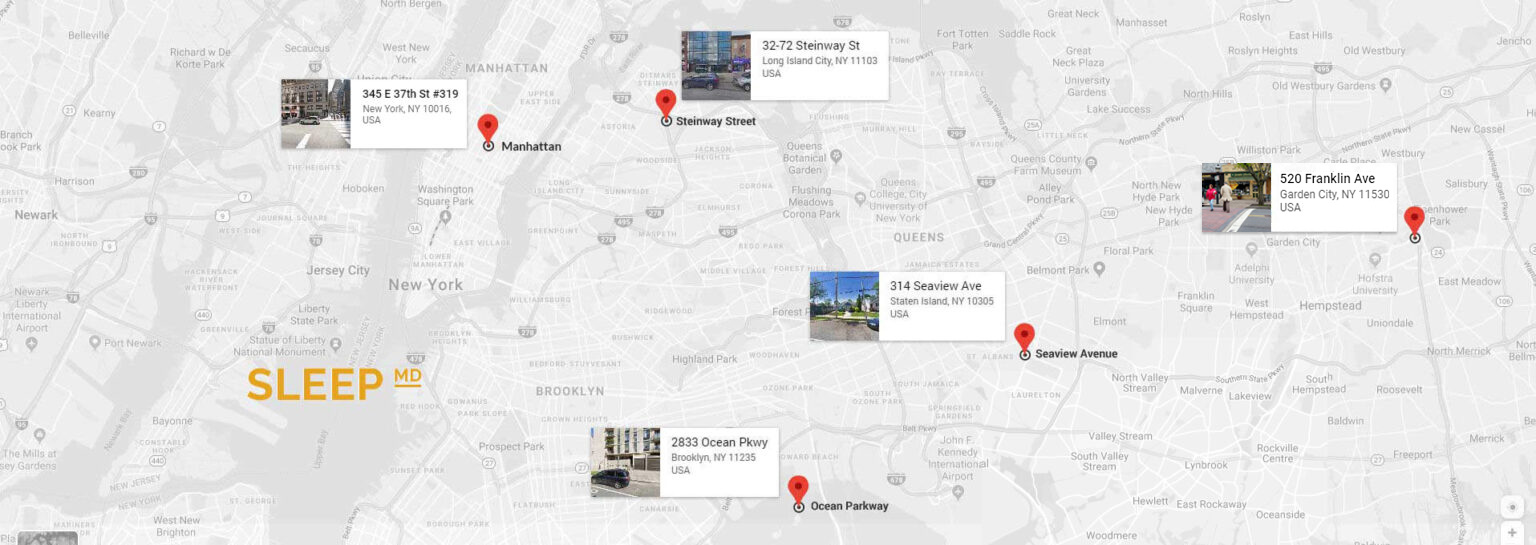
Request an Appointment Request an Appointment Name : Phone Number : Would you prefer us to text you or call? : TextCall Email Address : Date of Birth : Gender : — Select —MaleFemaleOther Location you would you like appointment? : — Select —ManhattanQueensStaten IslandBrooklyn Reason for Appointment? : — Select —Sleep Apnea issueInsomnia issueSnoring issueOther License : Front Back Insurance ID : Front Back Share any other information, you would like us to know : We have offices waiting to help you today in Manhattan, Brooklyn, Queens, Staten Island and Garden City Contact Us



 x
x